To save the sphincter is to save more than a muscle. It is to save dignity, normalcy, and the quiet freedom of a body that still answers to you.
When a person first hears the words "rectal cancer," a particular dread often follows close behind — not of the operation, but of a bag. Will I have to live with a stoma forever? It is one of the most common fears patients carry into my consulting room. And it is one I am most often able to set gently aside, because modern surgery can preserve the sphincter — and natural bowel control — in the great majority of people.
This guide explains it all, slowly and clearly: what the sphincter is, why it matters so deeply, how the special operations called LAR and ISR save it, and — just as important — how to care for yourself afterwards so that the muscle we worked so hard to preserve serves you well for life. Read it without hurry. Share it with your family. And take heart.
What is the anal sphincter — and why it matters
The anal sphincter is a ring of muscle that guards the very end of the bowel. It is the body's valve — the quiet gatekeeper that lets you hold stool and wind, and choose the moment to release them. We almost never think about it, until it is threatened. Only then do we realise how much of our dignity rests on this small, faithful muscle.
There are, in truth, two muscles working as one. The internal sphincter is involuntary — it stays closed on its own, without a thought from you, keeping the passage sealed at rest. The external sphincter is voluntary — the muscle you consciously squeeze to "hold on" when the urge arrives and a toilet is not yet near. Together with the pelvic floor, they create what doctors call continence and what you simply call control.
Here is why preserving it matters so much. To lose the sphincter is to lose that natural control — stool must then be diverted permanently to a stoma on the abdomen. To keep it is to keep the normal route, the normal rhythm, the normal life. That is why, whenever the cancer allows it safely, saving the sphincter is one of the most worthwhile goals in all of rectal surgery.
A Surgeon's Perspective
A sphincter is not just muscle — it is muscle and nerve together. A preserved sphincter that has lost its nerve supply will not work well. This is why good sphincter-preserving surgery is, above all, careful nerve-sparing surgery. We protect not only the muscle, but the delicate pelvic nerves that bring it to life.
How LAR and ISR preserve the sphincter
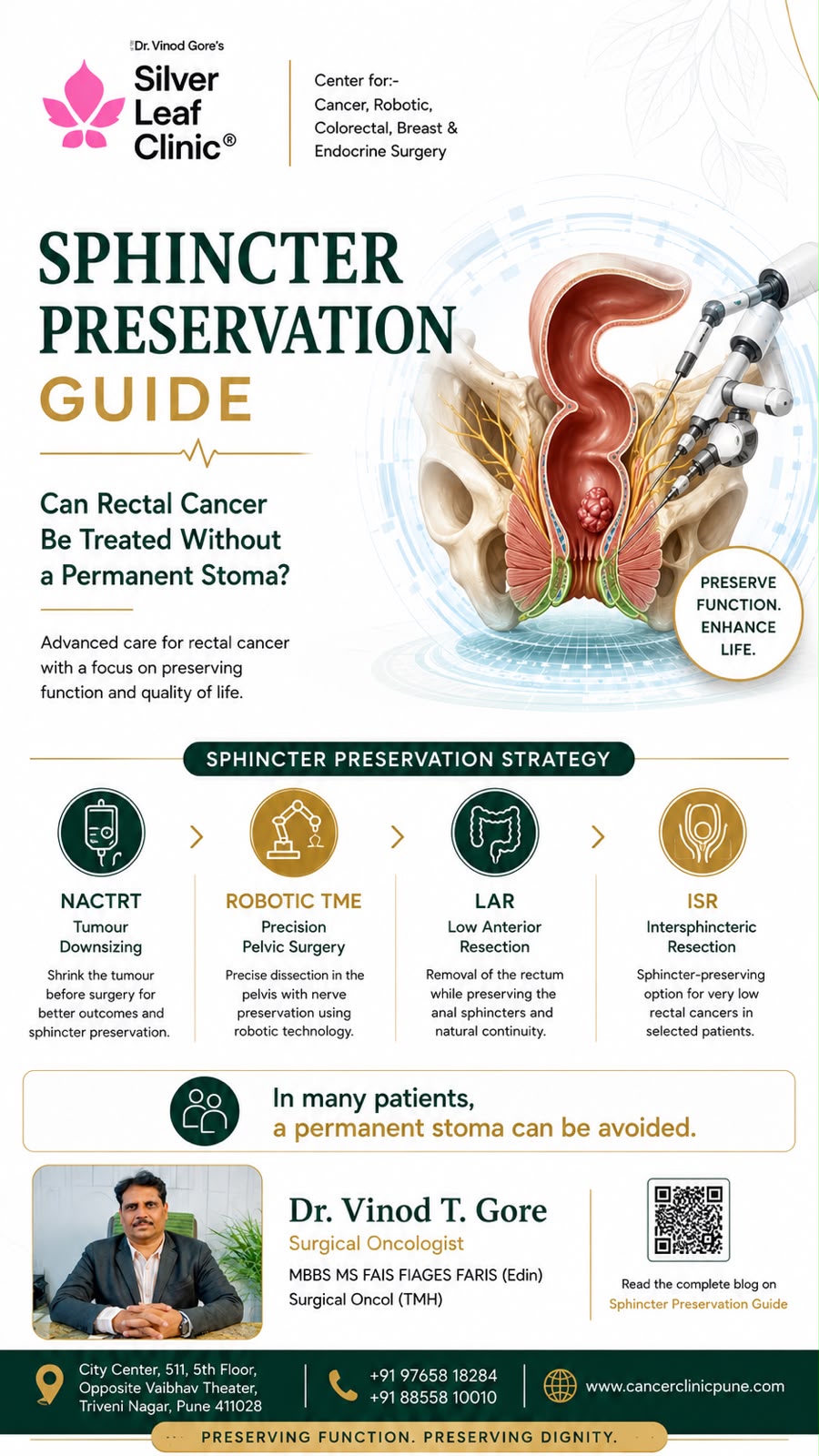
Curing rectal cancer means removing the tumour with a clear margin of healthy tissue all around and below it. The challenge is simple to state: the lower the tumour sits, the closer it lies to the sphincter, and the harder preservation becomes. The art of modern surgery is to remove the cancer completely while leaving the sphincter intact and working. Two operations make this possible.
LAR — Low Anterior Resection
For tumours in the upper and middle rectum, and many in the lower rectum, the surgeon removes the affected portion of the rectum together with its surrounding envelope of fat and lymph nodes (a step called total mesorectal excision, or TME), and then rejoins the colon to the remaining rectum or to the top of the anal canal. The sphincter is left untouched, and the natural route is preserved. To protect the fresh, low join while it heals, a temporary covering ileostomy is usually made — a small, planned stoma that is reversed a few months later. The stoma is temporary; the sphincter is saved.
ISR — Intersphincteric Resection
For very low tumours sitting close to the sphincter, where once a permanent stoma seemed the only answer, ISR offers another way. The surgeon removes the tumour along with the internal sphincter — the involuntary inner muscle — while carefully preserving the external sphincter, the voluntary muscle you squeeze. The colon is then joined directly to the anal canal. It is demanding, exacting work, often performed robotically for precision deep in the pelvis, and it saves natural control in patients who would otherwise have lost it. Like LAR, it is usually protected by a temporary ileostomy.
A Surgeon's Perspective
Sometimes the kindest, most curative step is to give chemotherapy and radiotherapy before surgery. This can shrink a low tumour away from the sphincter, opening a safe margin where there was none — turning an operation that once meant a permanent stoma into one that saves the sphincter. Cure always comes first; but with these tools, cure and preservation can far more often go together.
1
After Surgery
Healing & Rehabilitation
Saving the sphincter is the beginning of the story, not the end. The muscle and the bowel both need time and gentle help to settle into their new working pattern. With patience and the right rehabilitation, control improves steadily over the first one to two years — and most people arrive at a comfortable, predictable rhythm.
The first weeks — what to expect
In the early weeks after a low join (whether or not a temporary stoma is in place), and especially after the stoma is reversed, the bowel behaves differently than before. Many people notice frequency, urgency, and motions that come in clusters. This is common and has a name: LARS — Low Anterior Resection Syndrome. Please know in advance that this is expected, that it is not a sign anything has gone wrong, and that it improves. Knowing it is coming takes away much of its power to frighten.
The pillars of recovery
- Pelvic floor rehabilitation — the single most effective thing you can do (covered in detail below)
- A settled diet — eating in a way that gives your bowel a calm, predictable pattern
- Bowel retraining — gentle routines that re-teach control and timing
- Time and patience — the bowel adapts gradually; the trend over months is what matters
- Honest follow-up — we review your bowel function and adjust the plan together
2
Daily Care
Diet After Sphincter-Preserving Surgery
Diet is one of the most powerful tools you hold. The goal is not restriction for its own sake, but a calm, predictable bowel. In the first weeks, eat simply and introduce foods one at a time, learning how your own body answers each. Over the following months, most foods return — guided by what settles you and what unsettles you.
🍚 Settling & gentle
- Rice, well-cooked chapati, pasta
- Banana, peeled apple, ripe fruit
- Cooked, peeled vegetables
- Lean protein — chicken, fish, eggs, paneer
- Curd / yoghurt and probiotics
- Oats and other soluble fibre (firms output)
- Plenty of water through the day
⚠️ May loosen or hurry the bowel
- Very spicy, oily or fried foods
- Excess caffeine — strong tea, coffee
- Carbonated & very sugary drinks
- Large amounts of raw, high-fibre veg (early on)
- Alcohol
- Beans, onion, cabbage (gas)
- Very large meals — prefer smaller, regular ones
- Eat at regular times. A steady routine gives a steady bowel; skipping then overeating unsettles it.
- Keep a simple food-and-symptom diary in the early months. It quickly reveals your own personal triggers — which differ from person to person.
- Soluble fibre helps. Foods like oats, banana and white rice tend to firm and slow the output, easing urgency.
- Eat lighter in the evening to reduce night-time motions and rest better.
- Stay well hydrated — but spread fluids through the day rather than large amounts at once.
A gentle note on diet
- There is no single "stoma diet" or "sphincter diet" that fits everyone — your body is the guide
- Reintroduce one new food at a time, in small amounts, so you can read its effect clearly
- If a food clearly hurries or loosens you, pause it and try again weeks later — tolerance improves with time
3
The Heart of Recovery
Exercises & Bowel Retraining
If diet is one hand of recovery, pelvic floor exercise is the other — and of the two, exercise is the one that most directly rebuilds your control. The muscles that hold continence can be strengthened, just like any other muscle, through regular, patient practice. This is the work that, more than anything, turns a preserved sphincter into a sphincter that truly serves you.
Pelvic floor (sphincter) exercises — how to do them
These exercises strengthen the very muscles that give you control. They are simple, private, and can be done anywhere — sitting, standing or lying down. Ideally, learn them under the guidance of a physiotherapist, who can confirm you are using the right muscles.
- Find the muscle: imagine you are trying to stop yourself passing wind, and gently tighten and lift that muscle — without squeezing your buttocks, thighs or tummy.
- Slow holds: tighten, hold for a count of five (building towards ten), then relax fully for the same count. Repeat several times.
- Quick squeezes: a series of fast, firm tightens and releases, to build the muscle's quick response to urgency.
- Sets through the day: aim for three short sessions daily. Little and often, every day, beats long sessions now and then.
- Be patient: like any strength training, results build over weeks and months — not days.
Bowel retraining
Alongside the exercises, gentle bowel retraining re-teaches rhythm and control:
- Timed toileting — sitting at the same times each day (often after meals, when the bowel is naturally active) trains a predictable pattern.
- Don't rush, don't strain — give yourself unhurried, private time; straining works against you.
- Answer the urge sensibly — combine the "quick squeeze" to hold on with reaching the toilet calmly, rebuilding confidence.
- Medication if needed — simple bulking or anti-diarrhoeal medicines, guided by us, can steady things while the bowel adapts.
A Surgeon's Perspective
Patients sometimes feel disheartened in the first weeks, when control is at its most unsettled. I tell them all the same thing: judge your progress not week to week, but month to month. The bowel is learning a new way to work, and it learns steadily. Almost everyone who commits to pelvic floor exercise and a calm routine arrives at a good, manageable pattern.
4
Returning to Life
Activity & Living Well
As healing progresses, life returns — fully. The aim of saving the sphincter was always this: to let you go back to the ordinary, precious rhythms of living. Here is how to do it wisely.
- Walking can begin early and is excellent for recovery — start gently and build up.
- Avoid heavy lifting for the first several weeks to protect the healing abdomen and reduce hernia risk; then increase gradually.
- Return to exercise — yoga, cycling, swimming and the gym — once healed, building up step by step.
- Work — most people return within a few weeks to a couple of months, depending on how physical the job is. Knowing a toilet is nearby brings early confidence.
- Travel — entirely possible; plan toilet stops early on, and your confidence will grow with each trip.
- Social life and relationships continue fully. As control settles, the early caution fades and normal life resumes.
When to ask for help
⚠️ Speak to your surgeon or team if you have
- Severe or worsening urgency, leakage or frequency that is not improving with time and exercises
- Bleeding, severe pain, fever, or a swollen, painful abdomen
- Complete inability to pass stool or wind, with pain (possible obstruction)
- Bowel symptoms that are deeply affecting your mood, sleep or daily life — there is always more we can do
For stubborn symptoms, options such as specialised physiotherapy, biofeedback, transanal irrigation and nerve stimulation can help — you are never out of options, and never alone with it.
The truth worth holding on to
Let me return to where we began. The fear of a permanent bag is real, and almost every rectal cancer patient feels it. But for most people today, it need not come true. With careful surgery — LAR or ISR, often after treatment to shrink the tumour — the sphincter can be saved. And with patient rehabilitation, the right diet, daily pelvic floor exercise and a little time, the control you feared losing returns to a comfortable, livable rhythm.
The early weeks ask for patience. The months that follow reward it. You will eat well again, move freely again, work and travel and laugh again — and the surgery that once loomed so large will become a chapter you have closed, with your dignity and your ordinary life intact.
For further guidance
For patients facing rectal cancer surgery, or recovering from a sphincter-preserving operation, detailed assessment and support — including pelvic floor rehabilitation and management of bowel function — is available at Silver Leaf Clinic, Hadapsar. If you have been told you may need a permanent stoma, a specialist second opinion is genuinely worthwhile, because modern techniques save the sphincter far more often than before.
About the author: Dr. Vinod T. Gore is a surgical oncologist working in colorectal and gastrointestinal (GI) cancer surgery, sphincter-preservation and stoma surgery. He practises at Sahyadri Manipal Hospital and Silver Leaf Clinic, Hadapsar, Pune.
Correspondence: Silver Leaf Clinic, 511 City Centre, Solapur Road, Opp. Vaibhav Theatre, Hadapsar, Pune 411028 · ☎ 88558 10010
References & further reading
- Total Mesorectal Excision (TME) and sphincter-preserving surgery — colorectal surgical literature.
- Intersphincteric Resection (ISR) for low rectal cancer — outcome and technique reviews.
- Low Anterior Resection Syndrome (LARS) — assessment and management guidance.
- Pelvic floor rehabilitation and biofeedback in bowel function recovery.
- Neoadjuvant chemoradiotherapy in rectal cancer — downstaging and sphincter preservation.
This article is for general education and support. Every patient's surgery and recovery are different. Always follow the specific guidance of your treating surgeon, physiotherapist and care team.